For generations, women’s bodies have been treated as enigmas—mysterious, unpredictable, and, above all, less understood than men’s. When a woman walks into an emergency room clutching her chest, gasping for air, or collapsing from exhaustion, the response isn’t always swift action. It’s often a dismissive glance, a pat on the back, and a reassuring, “It’s probably just stress.” Heart attack symptoms in women are so routinely mislabeled as anxiety, panic, or exhaustion that the medical system has institutionalized a dangerous lie: women’s pain is psychological until proven otherwise.
The Myth of the “Hysterical Female”: A Historical Hangover
The roots of this systemic gaslighting run deep. The term “hysteria” was once a catch-all diagnosis for women’s ailments, a pseudo-scientific justification for dismissing their suffering as emotional rather than physical. While medicine has (theoretically) evolved, the echoes remain. Studies show that women are more likely to be misdiagnosed with anxiety disorders when presenting with cardiac symptoms, while men with identical complaints are rushed to the cath lab. This isn’t just a statistical anomaly—it’s a cultural inheritance. Our collective imagination still clings to the idea that women are prone to overreacting, that their bodies are less reliable than men’s. And so, when a woman describes chest pain that feels like a vise tightening around her ribs, or nausea so severe it leaves her doubled over, the default response is to reach for a prescription pad rather than a defibrillator.

The Invisible Symptoms: When Pain Wears a Different Mask
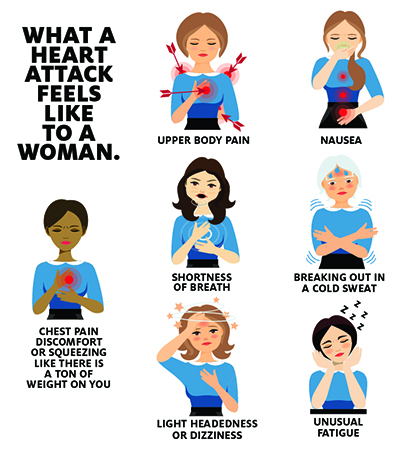
Men’s heart attacks are dramatic, cinematic—chest-clutching, jaw-grabbing, “Hollywood heart attack” territory. Women’s? They’re stealthy. Subtle. Invisible. Instead of crushing pain, a woman might feel a dull ache in her back, or a searing burn between her shoulder blades. Her jaw might throb. Her stomach might rebel. She might break out in a cold sweat, or feel a sudden, inexplicable fatigue that leaves her unable to lift her arms. These aren’t the symptoms we’ve been trained to recognize. They’re the ones we’ve been taught to ignore. And because they don’t fit the textbook mold, they’re labeled as “atypical”—a word that, in medical parlance, often means “not worth taking seriously.”
Consider the woman who collapses at her desk after weeks of dismissing her fatigue as “just burnout.” Or the one who’s told her dizziness is due to “low blood sugar” when, in reality, her coronary arteries are silently starving for oxygen. The medical establishment’s refusal to acknowledge these symptoms as cardiac in origin isn’t just negligent—it’s lethal. Women are 50% more likely to die from a heart attack than men, in part because their symptoms are so often misattributed to stress, depression, or hormonal fluctuations. The irony? The same hormones that make women’s symptoms harder to read are the ones that could save their lives—if only doctors bothered to listen.
The Gender Data Gap: Why Women’s Bodies Are a Medical Blind Spot
Clinical trials have historically excluded women, or included them in numbers so small that their data is statistically irrelevant. The result? A medical system built on male physiology, where women’s symptoms are either absent from research or lumped into vague categories like “non-specific chest pain.” Heart disease research has long focused on men, assuming their symptoms and risk factors apply universally. But the female heart is different. It’s smaller. Its arteries are more prone to spasms. Its electrical system is more erratic. And yet, when a woman’s heart misfires, we still default to the same tired narrative: it must be her imagination.
This isn’t just an academic oversight—it’s a public health crisis. Women are less likely to receive timely interventions like EKGs or stress tests, and when they do, the results are often misinterpreted. A woman’s troponin levels (a marker of heart damage) might rise more slowly than a man’s, leading to delayed diagnoses. Her pain might be dismissed as “functional” (a polite way of saying “it’s all in your head”). The gender data gap isn’t just a gap—it’s a chasm, and women are falling into it.

The Language of Dismissal: How Words Shape Women’s Survival
Language is power. The words doctors use to describe women’s symptoms shape how those symptoms are perceived—and whether they’re acted upon. When a woman says she feels “off,” she’s often met with a shrug and a suggestion to “take it easy.” When she describes “pressure” in her chest, she’s told it’s probably heartburn. The medical lexicon is riddled with euphemisms for women’s pain: “vague,” “atypical,” “non-specific.” These aren’t neutral terms. They’re weapons. They’re the linguistic equivalent of a doctor patting a woman on the head and sending her home with a Xanax prescription.
Consider the phrase “silent heart attack.” It’s a misnomer. There’s nothing silent about it—it’s just that women’s symptoms are so often unrecognized that by the time they’re diagnosed, the damage is done. Or take the term “angina equivalent,” a clinical way of saying, “We don’t know what’s wrong, but it’s probably not a heart attack.” These aren’t just clinical terms. They’re coping mechanisms for a system that would rather blame women for their own suffering than confront its own biases.
The Cost of Being Dismissed: From ER Delays to Preventable Deaths
The consequences of this dismissal are catastrophic. Women wait longer for treatment. They’re given weaker pain relief. They’re sent home with instructions to “rest and reduce stress” while their hearts continue to fail. The statistics are damning: women are 70% more likely to be misdiagnosed in the ER, and their mortality rates from heart disease are rising while men’s decline. This isn’t just a failure of medicine—it’s a failure of society. We’ve been conditioned to believe that women’s pain is less urgent, less real, less worthy of immediate action. And so, we die waiting for someone to take us seriously.
But the cost isn’t just measured in lives lost. It’s measured in trust eroded, in women who stop listening to their bodies because they’ve been taught that their pain doesn’t matter. It’s measured in the silent resignation of a generation of women who’ve been gaslit by a system that would rather call their heart attacks anxiety than admit it doesn’t know how to treat them.
What’s Next? Rewriting the Narrative on Women’s Heart Health
Change won’t come from within the system as it stands. It will come from women demanding better—from advocating for themselves, from refusing to accept “it’s just stress” as a diagnosis, from insisting on the tests they need. It will come from doctors unlearning the biases that have been drilled into them for decades. It will come from research that finally treats women’s bodies as more than an afterthought.
Until then, the myth persists: women’s heart attacks are anxiety. Their pain is psychological. Their suffering is a figment of their imagination. But the truth is far simpler—and far more damning. Women’s bodies are not mysteries. They are not hysterical. They are not broken. They are just different. And it’s time the medical system started treating them that way.







Leave a Comment